'Rugger Jersey' Finger (Flexor Digitorum Profundus Tendon avulsion)
|
The injury commonly referred to as ‘Rugger Jersey’ finger is a serious injury which usually occurs when the finger is caught in a jersey, shorts waste band or pocket. The main tendon that bends the finger (Flexor Digitorum Profundus) is pulled off (avulsed) from its attachment to the base of the last digit (distal phalanx). It requires early surgery to regain finger function, but unfortunately is commonly missed or ignored. Up until now, the injury was commonest in the ring finger of rugby players. Since the term was coined in the UK, ‘Rugger Jersey’ finger tends be used even though ‘Rugby Jersey” may be more appropriate in this country or maybe even more apt would be “Oztag finger”!
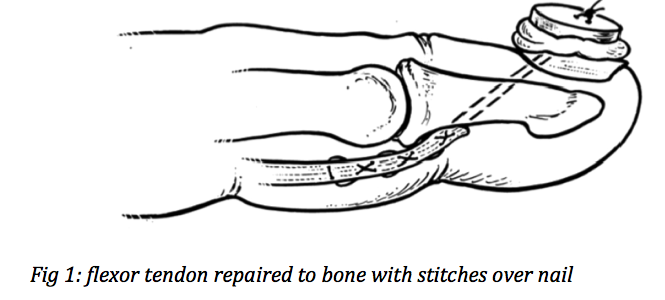
There are 2 flexor tendons (with muscles in the forearm) that run in a tendon sheath (tunnel) and bend each finger as well as an extensor tendon complex that straightens the finger joints. The intrinsic muscles and tendons contained in the hand assist and coordinate these functions. The Flexor Digitorum Profundus (FDP) tendon mainly bends the Distal Interphalangeal Joint (DIP) and is the strongest and most important flexor. The Flexor Digitorum Superficialis (FDS) bends the Proximal Interphalangeal Joint (PIP). In the little finger the FDS is often absent or very small and weak. When a finger is hyperextended at the same time that the muscle is forcibly contracting it can be powerful enough to rupture the weakest point; the tendon insertion to bone. This causes pain, swelling and the inability to bend the tip of the finger. Because the proximal joint still bends from the intact FDS tendon, the injury can easily be missed without careful examination. When the reverse happens, an extensor tendon avulsion can occur (‘Mallet Finger’); though this still requires treatment it is not as serious and can often be managed successfully without an operation. The tendon needs to be repaired to bone as soon as possible (within 1-2 weeks); the muscle pulls the tendon into the palm and later repair can be too tight and therefore not only adversely affect the function of the finger, but the whole hand. The exception is when there is a bone fragment attached to the fragment, which gets stuck in the tendon sheath preventing further retraction; repair in this case can be effective up to about 6 weeks. The whole finger (and sometimes palm) usually needs to be opened surgically to find the tendon end, pass it back through the sheath and then the tendon can be securely stitched back to bone using various methods. The tried and tested method is to suture through or around the bone and over the nail, with a button for comfort, pulling the tendon snuggly into its bony insertion. The tendon needs to heal back to the bone, taking approximately 3 months to regain full strength, but there is enough healing after 6- 8 weeks to remove the button and suture. It is important that the repair is strong enough to allow early movement within a splint, with the guidance and supervision of an experienced physiotherapist or hand therapist. Movement prevents the tendon from getting scarred and stuck in the sheath and minimizes finger stiffness. As alluded to above, the majority of these injuries I see now are from Oztag though other contact ball sports including netball are also a common cause. Depending on the mechanism of the injury, Oztag (and other football players) sustain many complex fractures that require expedient treatment and sometimes surgery to achieve a good functional result. The biggest problem with finger injuries is long term stiffness; this commonly effects the function of the whole hand and can make continuing sports and work endeavours difficult or impossible. The key to avoiding a poor result from sports finger injuries is early presentation and recognition of the injury and avoid thinking it is ‘just a sprain’ until more serious causes have been excluded. |


|
